(We’re a team of Harvard students working with Centers for Medicare & Medicaid Services (CMS) and the Social Security Administration (SSA) to improve the Medicare enrollment process for people turning 65 years old—and this is our fourth and final blog post.)
Larry is turning 65 in a few months. He knows he has to sign up for Medicare, but that's about the extent of his knowledge. He called the Medicare phone number, only to be directed to the Social Security number, who instructed him to call a Medicare number. Frustrated, he went online to Medicare.gov, but gave up after 10 minutes. Larry was overwhelmed by thousands of webpages and the terminology and acronyms he didn’t understand, like part A, Medigap, and OM. He was annoyed and worried. His health isn't great, and he doesn't want to be uninsured—especially during the pandemic.
A couple of months later, Larry retired and lost his health insurance. He misses the deadline to sign up for Medicare because he had to wait months for an in-person appointment. Now, Larry is uninsured and worried. He faces lifetime penalties for not signing up for Medicare on time. Larry feels lost.
Larry was one of the first people we interviewed as part of our semester-long project with CMS and SSA to improve the initial Medicare enrollment process. (His name has been changed to protect his privacy.) While Larry’s situation may be unique to him, his concerns are not, and we have heard similar anecdotes from many people we interviewed.
Larry and others are confused about how to start the enrollment process. Many have been lucky to have health insurance covered by their employers and haven’t had to think about health insurance for the past 40 years, but now what? They are overwhelmed with the amount of information in disparate locations—from websites to mailings to instruction manuals. They are frustrated with the long wait times for phone calls and in-person visits. And they are unsure what actions are required from them and when they need to make decisions.
What We Built
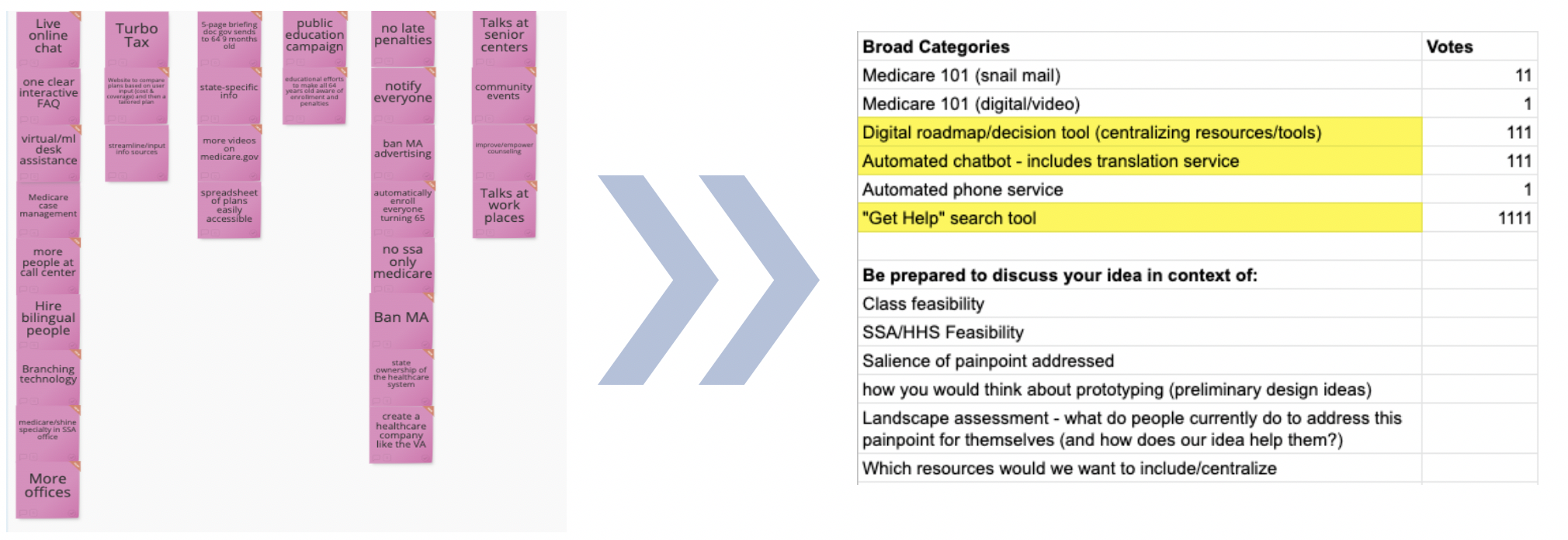
We listened to over 40 interviewees, and based on their input, brainstormed 30 potential solutions. Considering feasibility and scale, we built three tools to tackle the challenges enrollees face: a Medicare roadmap tool, a get help website, and a chatbot.

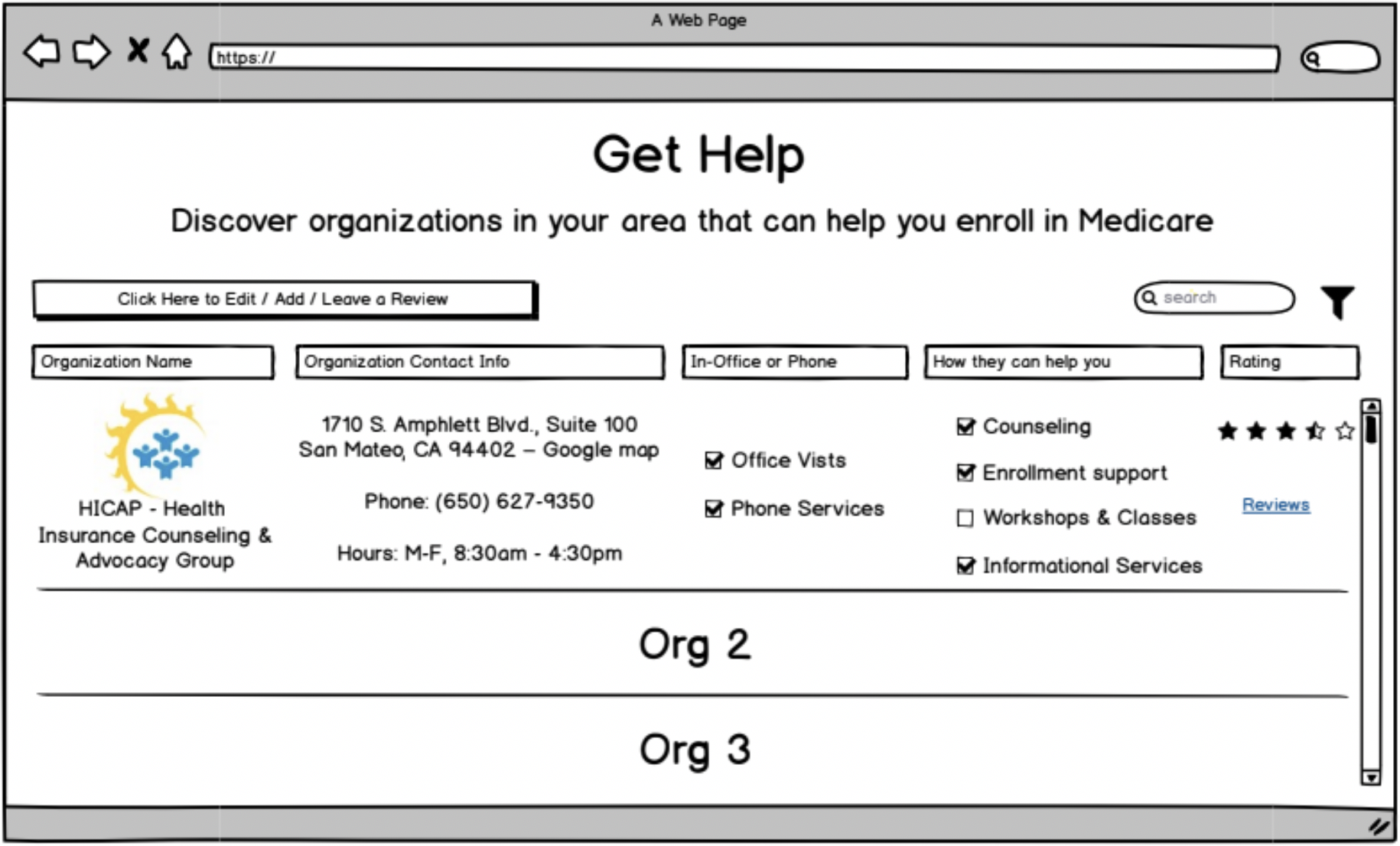
Our initial drawings translated to simple online versions
To get real human feedback, we tested our simple paper and digital prototypes, seen above, with people aged 63 and older. They had an overwhelming preference for the Medicare Roadmap prototype, which inspired our team to focus on further refining the tool.
The Medicare Roadmap
The purpose of our proposed Medicare Roadmap tool is to give people like Larry a clear starting point and personalized plan to navigate the Medicare enrollment process step-by-step. After testing the roadmap with an additional 48 prospective Medicare enrollees, current Medicare beneficiaries, and other people involved in the broader ecosystem (e.g. SSA regional office employees), we made several improvements. Below is a screenshot of our final product.

Starting screen from our Medicare Roadmap prototype
The tool allows people to answer a series of questions in order to determine:
When they are eligible for Medicare;
When they can enroll in Medicare;
Which Medicare coverage options are available;
What steps to take to apply for Medicare.
The tool aims to break down each step of the process into an easily digestible format with an emphasis on making it easy for everyone to understand.
After responding to the questions on the Medicare Roadmap tool, the applicant is presented with customized and detailed healthcare plan information, as well as a personalized application checklist. The tool gives people the necessary information, as well as clear steps, to determine the criteria needed to decide which healthcare plan is best for them.

Checklist screen from our Medicare Roadmap prototype
What about Larry?
Larry never left our hearts or minds, so we called him back later in the course and showed him our Medicare Roadmap tool. His response? “I definitely would use this tool because it makes it much more clear and asks important questions so you don’t need to go through extra steps to find the answer for yourself.” Larry said with a sigh of relief.
We hope CMS and SSA will use our idea of a roadmap to provide everyone a simpler, easier, and more enjoyable experience enrolling in Medicare.
Thank You
Thank you to Robert Teller, Benno Schmidt, Misu Tasnim and Jessica Weeden from SSA and CMS for partnering with us on this important project, and all the people across SSA and CMS who gave us their time and advice as we developed these solutions. It was an honor to work with you all and be inspired by your passion for public service.
And thank you to all of our interviewees—who could more accurately be called our co-creators—who shared their opinions, experiences, and preferences. We hope our solutions make your experiences with Medicare enrollment better!
—Christina Wu, Gwendolyn Lee, Melia Henderson, Mia Li, Rob MacGregor